I don't know. I have no experience with this injury.


 Member
Member




I've been back 2 months after a 5 month recovery from the surgery.
I was wondering if I have anything to worry about as my cleans get heavier. Have you ever heard of this injury being caused by the lift?
It had a very fast onset previously (2 days and half my hand was permenantly asleep).
I had severe muscle wastage of (forgive me for not knowing its name) the muscle between your thumb and hand which is just starting to grow back...
Do you think I have anything to worry about proceeding with heavier weights?
 TMPHBITEU
TMPHBITEU
I don't know. I have no experience with this injury.
Member
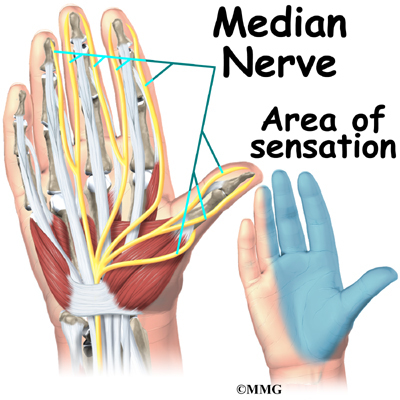
I don't know about the procedure you had, but on the ventral (palmar) side of your hand the thumb, pointer, and middle finger are innervated by your median nerve, not your ulnar nerve -- what you're describing is what can be seen in really bad carpal tunnel syndrome where the median nerve is what gets fried.
Sounds like if anything it would affect your ability to achieve a heavy grip. It also might result in "ulnar deviation" of the hand, i.e. because you have more ulnar than median nerve input your hand deviates at the wrist towards the 'pinky' side and not the thumb side.
If there isn't some surgical reason why lifting is contraindicated it sounds like only experimenting with heavier weights will tell you to what degree grip strength and hand positioning is a limiting factor.
Member
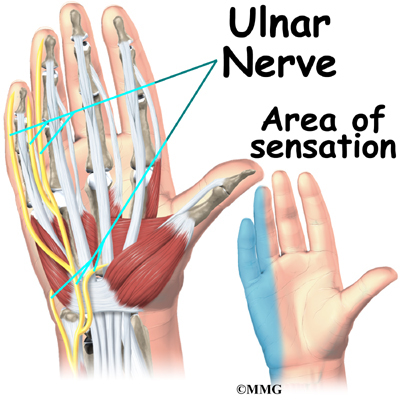
I am aware of the side of the hand the ulnar controls sensation to (your pinky and half your ring finger) however, it also controls the muscle I mentioned above.Originally Posted by Paul1

http://www.tannershand.com/
see the above link to get a better understanding of the condition.
Member
Edge,
We should just mention in follow up that we had a private conversation about this, and there are fundamentally incorrect things in the link you've attached.
The neuroanatomy of the hand is pretty straightforward; the neuroanatomy of the whole upper extremity is a pain in the ass, and it's the bane of every first year med student's existence to memorize it.
It should be mentioned that ATROPHY of a muscle due to a neurologic problem is most often due to a lower motor neuron disease -- i.e. anywhere between where the nerve roots leave the spinal cord and where the nerve endings reach the muscle. Upper motor neuron diseases (i.e. injuries to the brain or the spinal cord) do not directly cause atrophy (though atrophy from disuse will eventually happen).
So if you see atrophy, the doctor's job is to figure out where a nerve lesion is.
To simplify, the hand is innervated by three major nerves.
The ventral (palm) side of the hand is innervated by:
-The ulnar nerve, which supplies both motor and sensation to the 4th and 5th fingers (ring finger and pinky) and the hypothenar muscles (the fleshy part of the hand under the pinky)
-The median nerve, which supplies the 1st-3rd fingers (thumb through middle finger) and the thenar muscles (the muscles of the palm itself)
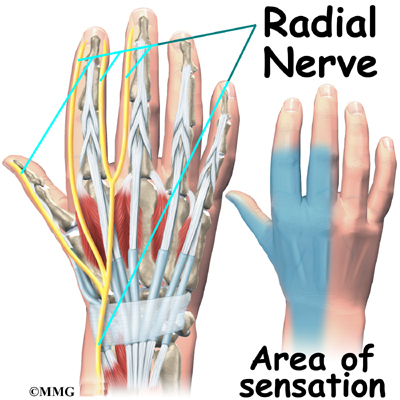
The dorsal (back) side of the hand is innervated by the radial nerve
These three nerves originate from nerve roots that leave the cervical spinal cord, if I recall correctly it's cervical spinal nerves 2 through 8. Parenthetically the innervation to your diaphragm also comes from here.
After leaving the spinal cord the cervical nerve root fibers merge in a horribly complicated way as they pass through your upper thorax and armpit, and this pathway of nerve organization is called your brachial plexus.
Anyway, there are two fairly common syndromes that lead to atrophy of the hand muscles. One is damage to or entrapment of the median nerve. The most common cause of this is carpal tunnel syndrome, because it is the median nerve that passes through the carpal tunnel. Entrapment of this nerve by inflammation of the carpal tunnel (or of the retinaculum, the fibrous tissue that surrounds the wrist), can lead to atrophy of the PALM, weakness flexing the thumb / pointer / middle finger, and numbness or tingling on the ventral (palmar) side of those fingers. If that is the disease, then you cannot blame it on the ulnar nerve, like the person in that link did -- he's wrong and his neurologist was right. The ulnar nerve CAN be entrapped, though, especially as it passes around the elbow. This is the 'funny bone' where the ulnar nerve is quite vulnerable -- and if you smash your 'funny bone' you'll go numb on your pinky and ring finger, exactly where the ulnar nerve does its business. "Cubital tunnel" syndrome refers to compromise of the ulnar nerve as it passes around the elbow.
Beyond that, if there is atrophy, weakness, or "paresthesias" (numbness, burning, tingling sensation) in the distribution of multiple nerves, there is a whole list of possibilities that have to be sorted out. It could be a nerve root problem (aka "radiculopathy"), like from cervical disk disease. It could be a brachial plexus problem -- things like injuries to the armpit or tumors in the armpit can do this. It might not be an anatomical problem at all -- for instance diabetics can get neuropathy affecting multiple nerves all over their body, as can an enormous list of people with other diseases.
So anyway for MANY people there will be a simple explanation like a median or ulnar nerve issue -- but not always, and there is no substitute for having a doc who understands (and can examine) this stuff take a real look.
Hopefully that explanation isn't bad (for a germ doc).
TMPHBITEU
It's apparently much better than any other explanation he's been given. I like it too.
Member
Are you referring to Edge's diagnosis or the diagnosis in the link he posted? They are different people.
He would have to have a really abnormal amount of crossover of the ulnar nerve to the thenar eminence for that to make sense, it really doesn't reconcile with the neuroanatomy of the hand. There must have been more compelling evidence than just thenar wasting to support the diagnosis of an ulnar nerve problem -- you'd expect paresthesias or weakness of digits 4 and 5, or ulnar deviation of the hand. But whatever the evidence was it sounds like he got a procedure that worked, which in the end is what mattered.
TMPHBITEU
I was referring to your excellent explanation of hand neuroanatomy. Now, let's hope MMG doesn't sue us for the use of these excellent graphics. You're very odd at times.
Member
Gotcha, thanks. I thought you were just fucking with me.
Member

A nerve conductivity test was performed, an mri, and an ultra sound. It was cubital tunnel syndrome causing the issues and the muscle wastage. I had the operation for it in December 2012. My surgical follow up is tomorrow and I will ask what the name of the muscle that disappeared is. The sensation diagrams are exactly what I had, but the muscle wastage was on the other side (which is apparently very normal and happens in almost all cases). Whatever the muscle is which allows you to keep your index finger spread open.
I'll update ya tomorrow seeing as you were kind enough to give such a detsiled response.
 Posting Permissions
Posting Permissions