You'll have to post better graphics, these are too small to read.


 Member
Member




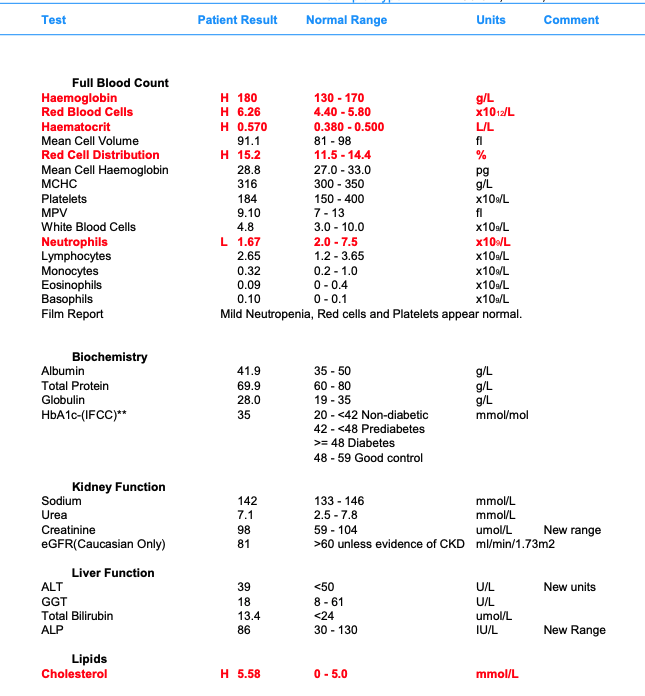
Hey Rip, me again. I posted up 3 months back with some concerns regarding my bloodwork. Yourself & Dr . Nichols kindly put my brain at ease. I just had my 6 month bloods done & some other markers are now raising, my clinic has advised me to completely stop treatment until I can donate some blood (I've tried 4 times already here in the UK and they canceled on me each time). I have been feeling pretty shit recently and I think the estrogen is certainly helping out with that, currently on 2 pumps of 75mg/ml versabase cream daily and 2x weekly HCG shots (0.1ml).
Any thoughts on this, I'm a little concerned with completely stopping treatment?
32m - 215lbs - 6ft
Screenshot 2022-09-22 at 12.57.18.jpgScreenshot 2022-09-22 at 12.57.13.jpg

 TMPHBITEU
TMPHBITEU
You'll have to post better graphics, these are too small to read.
Member
I recommend listening to the podcast where we discussed the secondary erythrocytosis from testosterone therapy:Originally Posted by Uhtred

Testosterone Therapy as a cause of Secondary Erythrocytosis
The most common side effect of testosterone therapy, and the one that causes the most concern for the patient and their family physician, is a secondary erythrocytosis which is an increase in red blood cells. It is often described by the patient and their physician as “thick blood” requiring a blood donation because they fear it could possibly lead to a heart attack, stroke, or blood clot.
Where does this fear originate? When the family physician or internist sees an increase in red blood cells along with hemoglobin and hematocrit, it is frequently misinterpreted as the patient having Polycythemia Vera which is a myeloproliferative neoplasm of the bone marrow (bone marrow cancer). Thrombosis (blood clots) are a leading cause of morbidity and mortality in this disorder. Polycythemia vera is known as a primary erythrocytosis where there is an unregulated proliferation of hematopoietic clonal stem cells which leads to over production of red blood cells, white blood cells, and platelets. In Polycythemia Vera, in contrast to the secondary erythrocytosis from testosterone therapy, not only is there a quantitative change in the number of circulating blood cells, but there is also a qualitative change that leads to the expression of procoagulant characteristics. In addition there are abnormalities involving the vascular endothelial cells which become procoagulant in response to inflammatory stimuli. These abnormalities result in a hypercoagulable state leading to an increase in arterial thrombosis and venous thrombosis. Therefore part of the recommended treatment is blood donation to reduce the risk of thrombosis. The risk of elevated hematocrit seen in patients with polycythemia vera cannot be extrapolated to hematocrit elevation seen during testosterone therapy. They are not the same and should not be treated as such.
The secondary erythrocytosis from testosterone therapy is an increase in red blood cells only leading to an increase in hemoglobin and hematocrit. The mechanisms behind testosterone stimulating red blood cell production is not completely understood but is thought to occur through stimulation of erythropoietin, stimulation of hematopoietic progenitor cells, and reduced hepcidin. A secondary erythrocytosis is also seen in other conditions such as smoking, obstructive sleep apnea, chronic obstructive pulmonary disease, and living at high altitude. While a primary erythrocytosis has been well established as a risk factor for thromboembolic disease the risk of a secondary erythrocytosis has not been shown to cause an increase in thromboembolic events in any randomized control trial or prospective study to date. Most guidelines recommend following hematocrit after initiating testosterone therapy and if the Hct exceeds 54% clinicians should either adjust testosterone dosage, stop therapy, order phlebotomy, or recommend a combination of these. These recommendations are based on assumptions and the Hct cut off of 54% was arbitrarily chosen and not based on any study showing harm when this value is exceeded with testosterone therapy. The upper limit of normal for hematocrit in most laboratory reference ranges for healthy adult males is 54% which is where this value is likely derived. This is a normal range for men without a secondary erythrocytosis and not for men on testosterone or living at high altitude for instance. There are over 80 million people that live higher than 2,500 meters and they develop a secondary erythrocytosis. Men in parts of Bolivia for instance have a normal range of Hct from 45-61%. These men are not at an increased risk of thrombotic events nor do they have to undergo phlebotomies to manage their hematocrit. One also cannot ignore the observation that literally tens of thousands of men presently use and abuse testosterone in this country and have done so for decades. A large percentage of these men are not under the supervision of a physician or getting lab work and yet we have not seen an epidemic of heart attacks, strokes, or blood clots in these men. Almost all previously reported cases of testosterone treatment related venous thromboembolism were seen in patients with a previously undiagnosed thrombophilia like factor five Leiden deficiency.
The other concern with increasing hematocrit is that it will increase viscosity and decrease blood flow resulting in thrombotic events. In experimental studies using rigid glass viscometers or cone-plate viscometers there is a logarithmic increase in viscosity with increasing hematocrit. It is inappropriate to correlate these in vitro viscosity readings to what occurs to flowing blood through tiny distensible vessels in vivo. In other words, viscometer measures in these experiments do not translate to human blood vessels. Firstly, the flow through these narrow blood vessels is rapid (high shear rate), which in a non-Newtonian fluid such as blood causes a marked decrease in viscosity. Second, blood flowing through these narrow channels is axial with a central core of packed red blood cells sliding over a peripheral layer of lubricating low viscosity plasma. With a secondary erythrocytosis there is an increase in blood volume which enlarges the vascular bed, decreases peripheral resistance and increases cardiac output. Therefore, in a secondary erythrocytosis optimal oxygen transport with increased blood volume occurs at a higher hematocrit value than with a normal blood volume. A moderate increase in hematocrit may be beneficial despite the increased viscosity
Testosterone also exerts multiple beneficial effects on the vasculature and its components which may protect against thrombosis. In other words testosterone has positive effects on vascular reactivity.
Testosterone is a vasodilator and increases nitric oxide
T decreases plasma concentrations of pro coagulatory substances
T improves erythrocyte membrane lipid composition and fluidity
T increases red blood cell deformability
T reduces levels of lipoprotein a
Donating blood to reduce hematocrit may also provide men with a false sense of security.
In a study done over a two-year period of time they looked at men who donated blood that were on testosterone therapy at least 25% of them had a hematocrit about 54% and when they came back for repeat donations 44% of them had a persistent elevation of hematocrit above 54%. So it essentially showed that repeat donations were insufficient to maintain a hematocrit below 54%.
Testosterone therapy was first used clinically 1937 and it has been used in thousands of randomized control trials. There is not a single randomized control trial to date that shows an increased risk of major adverse cardiac events with testosterone therapy.
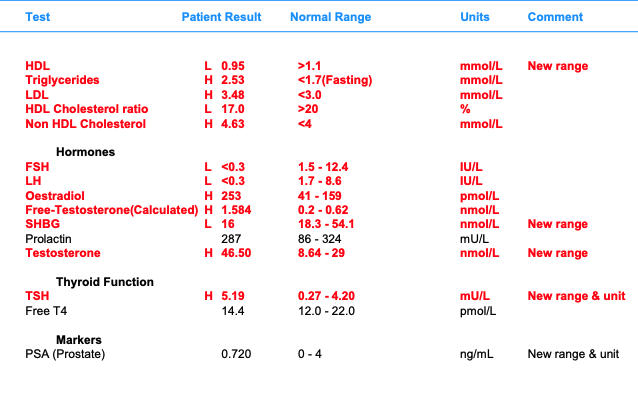
Also, the clinic obviously doesn't know a lot about what they're doing because you're wasting your money getting an FSH and LH level in somebody on testosterone. They're going to be suppressed. The estradiol measure wasn't the sensitive test no it is not accurate. You also have to know how I feel about measuring estradiol in a man. Most men feel better off of hCG than on hCG. There is no need to stop treatment and if I had to stop treatment on every man who had a secondary erythrocytosis then I would have to stop it on everyone for the most part because that is the most common side effect from testosterone and has never caused harm in any study.
J. Keith Nichols MD
Member
Sorry Rip, same thing happened last time, this should be easier to see now.
@Dr Nichols I really appreciate the level of detail you provided here. I have listened to the podcast twice already but I will still probably get value from another go. I agree with you regarding my clinic, unfortunately here in the UK we're very limited with our options, there are honestly a handful (I think only 2-3) private clinics that provide TRT. The NHS is a complete no-go, they think a 30 yo male with a total t of 10 nmol/L is okay and all my symptoms are not a problem.
I shall bring this up with the Dr, I said to him I simply will not just come off so he said I could reduce my dose to once a day until I donate blood, needless to say I'll continue as normal but will donate just to appease him.
So if someone is experiencing what we believe to be high E symptoms (sore nipple, irritable, anxious etc) there's still no value in looking into that? I'm not contesting that I'm just curious on what I should do about these symptoms I have currently. I may come off the HCG, but given my age I do have fertility concerns, from what I've read people have mixed opinions on whether starting HCG/HMG later down the road will be an issue, so decided to run HCG along with the test just incase.
Member
Im also interested in Dr. Nichols thoughts on HCG for a man who is concerned about fertility.
Member
This response should be made into an article or another linkable citation for future use when this question inevitably comes up again on this forum.
This may be tangential to the thread, but do the qualitative changes in blood cells/plasma seen in primary erythrocytosis mean there is an increased risk of blood clots or other problems for patients who receive blood donated by people with polycythemia vera?
Member
First of all whenever you start testosterone therapy its going to take some time for your body to acclimate. So some initial side effects you may be experiencing will usually resolve with time. Most men want to make changes too quickly before they give their body the chance to acclimate. If we were to somehow be able to raise our testosterone levels naturally to an optimal level that would occur over time and our body would acclimate naturally. The problem with testosterone therapy is that we raise our levels quickly and that can call some initial side effects that will resolve with Time And almost every individual. Everything gets blamed on Estradiol. Also, all the hormones work synergistically and I find it best to optimize all the hormones along with testosterone. In addition, a lot of your problems are not testosterone related because you in fact have hypothyroidism based on your most recent lab studies. A lot of men do not feel better when they get on testosterone therapy because the symptoms of testosterone deficiency and thyroid deficiency overlap in many areas. A lot of clinics are throwing testosterone at what is in fact a thyroid problem. Thats why you need to have someone look at all of your hormones and make recommendations based on symptoms and levels of each hormone. If you look at the package insert for human chorionic gonadotropin you will see some of the problems youre experiencing as a side effect.
With regard to fertility. Yes you can start hCG along with testosterone but a lot of men choose to start testosterone in isolation and when they are ready to father a child they will then add hCG to their testosterone or discontinue their testosterone for a period of time and utilize only hCG and clomid for instance until the pregnancy is obtained. So a man can use hCG or Clomid in place of testosterone to maintain fertility, they can utilize testosterone along with hCG to maintain fertility, or they can use testosterone initially and then when theyre ready to father a child add hCG and or Clomid. So there are options depending on the individuals personal preferences.
If a man wants to have a child in the immediate future then its best not to utilize testosterone but instead utilize hCG or Clomid as mono therapy. The problem is most men dont feel good on hCG or clomid model therapy. Other options would be to utilize hCG along with testosterone which will maintain fertility and once the pregnancy is obtained then they can discontinue the hCG. Other options would be to utilize testosterone in isolation and then once someone is ready for pregnancy they can then add hCG and or Clomid or even HMG if necessary and even consider discontinuing testosterone and told a pregnancy is obtained. So there are various options that one can discuss with their provider and make the best decision for them and their family
What you were reading is a initial rough draft of a review article I am writing on the topic. Blood is usually tested for an increase in hematocrit and platelets to rule out disorders like polycythemia vera before people are allowed to donate. I will provide Mark with the finished article with all the references once it is completed so that he can provide it to starting strength members
Member
Dr. Nichols where would you suggest Clinicians wanting to learn more about TRT should start? I read Dr. Rouzier's book but that was more or less for the general public. Worldlink medical has a 4 part series that can lead to a certification that I am considering but there is considerable cost, I may end up doing it this fall. Appreciate any advice, thank you.
Member
Save yourself a lot of wasted time and money elsewhere and just take the plunge and do Part 1 of the WorldLink medical conferences. That will be the absolute biggest bang for the buck and you will truly be learning evidence-based medicine. I just returned from lecturing at part 5 which is called hormones and beyond.
Member

Excellent, thank you for your feedback I'll sign up for part I and see where it takes me. I work largely in addictions and this population in particular seems predisposed to and undertreated for hypogonadism. Appreciate your in-depth explanations regarding common TRT controversies.
 Posting Permissions
Posting Permissions